
COPD Statistics & Facts (2024): How Common Is COPD?

Report Highlights:
- Every year, over 150,000 Americans die of chronic obstructive pulmonary disease (COPD), which equals one death every 4 minutes [9].
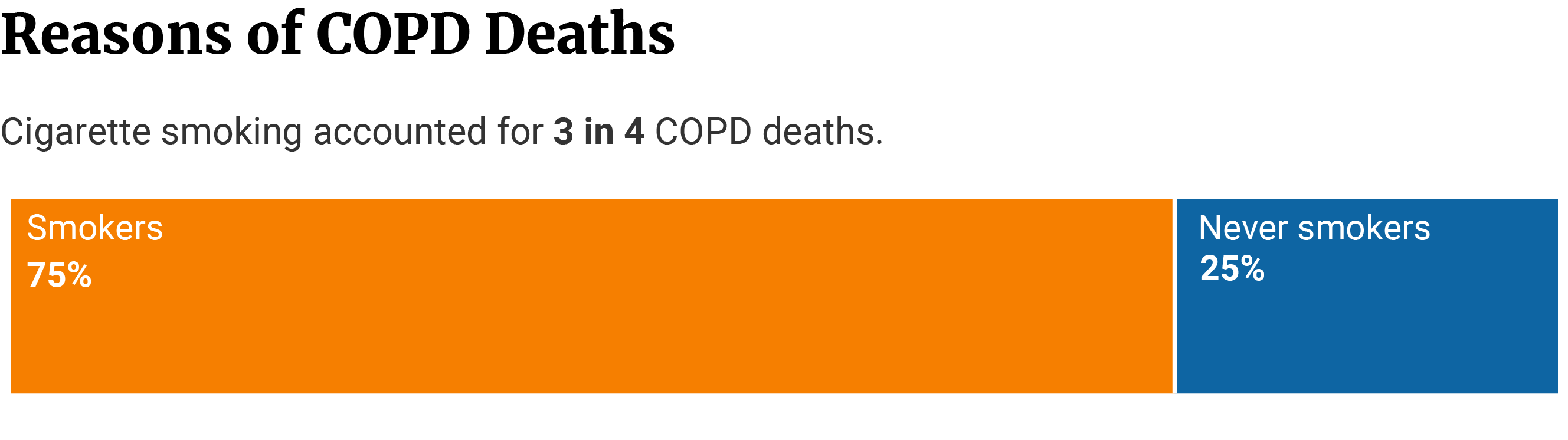
- Smoking tobacco causes 75% of COPD deaths, while 25% of the people diagnosed with this condition have never smoked [9].
- People who have never smoked cigarettes in the last 30 days have a 67% lower COPD prevalence, while former users and cigar users have a 43% and 54% lower prevalence of COPD, respectively [37].
- In 2019, COPD was the third principal cause of death globally at 5.8%, right behind stroke and ischaemic heart disease [13].
- The average age at death from COPD between 2000 and 2005 was 76.6 years compared to 72.9 years in 1980-85 [4].
- 7.3% of COPD patients will live 15 years after admission for worsening COPD compared to 40.6% of the general population of the same age and sex [46].
- Hospitalized COPD patients have an 82% lower survival rate in the next 15 years after admission for worsening COPD than people in the general population [46].
- COPD is more prevalent in females at 7.1% than in males at 5.7% because women smokers have a 50% greater likelihood of developing COPD than men [2, 3].
- According to a Danish study, it takes 25 years of smoking to develop COPD. The data shows that at least 25% of smokers who had no COPD symptoms will develop clinically significant COPD [23].
- On average, it takes three to five months for the patient to learn whether they qualify for COPD disability and an additional five months to receive the first payment [7].
Chronic obstructive pulmonary disease (short: COPD) encompasses several chronic respiratory diseases characterized by airflow blockage and difficulty breathing [28].
The two main conditions that fall under the term COPD are chronic bronchitis and emphysema. Together with asthma, all these conditions (including COPD) are known as chronic lower respiratory diseases (CLRD) [20].
We’ve gathered the most interesting and helpful statistics about COPD to shed light on this condition.
COPD Prevalence & Mortality Demographics and Statistics
In the United States, every 46.3 deaths out of 100,000 people are attributed to COPD [5].
![]()

According to the World Health Organization, 3.23 million people died of COPD in 2019 — making this condition the third leading cause of death globally [8].
Millions of people around the globe die from COPD every year, as this disease remains a significant global burden. It’s alarming that this condition remains undiagnosed and untreated in millions more.
How Many Deaths Does COPD Cause?
More than 150,000 Americans lose their lives from COPD within a year, which equals one death every 4 minutes [9].
![]()

The total number of deaths from chronic lower respiratory diseases (CLRD) was higher in 2018 than in 2020. In 2020, 152,657 people died of CLRD compared to 2018 at 159,486, making these conditions the sixth and fourth main cause of death in the US, respectively [5].
![]()

In 2017, 160,201 people died of COPD, making it the year with the most deaths from 1999 through 2020. This year is followed by 2018 with 159,486 deaths and 2019 with 156,979 deaths. Among the top five years of death from COPD are 2015, with 155,041 people, and 2016 with 154,596 people [5].
In 2004, 121,987 people died of COPD, making it the year with the lowest number of deaths between 1999 and 2020. With 122,009 and 123, 013 COPD deaths, 2000 and 2001 follow suit, respectively [5].
Compared to 1999, 28,476 more people died of COPD in 2020, which shows the increase in the number of deaths within this period [5].
8,924 more people have died of COPD in 2005 than in 2000, while 7,147 more died in 2010 than 2005. In 2015, 16,961 more people lost their lives to COPD than in 2010, while fewer people (2,384) died of COPD in 2020 than in 2015 [5].
Most (85.58%) COPD deaths occur among those aged 65 years or older with a total of 2.6 million deaths from 1999 through 2020 [5].
COPD Mortality Statistics In the United States
COPD is a principal cause of mortality and morbidity in the United States. The average age at death from COPD in the period between 2000-05 was 76.6 years [4]. The main cause of COPD and COPD deaths is tobacco smoking [40].
What’s the Average Age At Death from COPD?
Between the 1980-85 period, the average age at death from COPD was 72.9 years, while between 2000-05, it rose to 76.6 years. The 3.7 age increase indicates that COPD patients don’t die as young as four decades ago. This may be connected to early diagnosis, prompt treatment, and a decline in tobacco smoking [4].
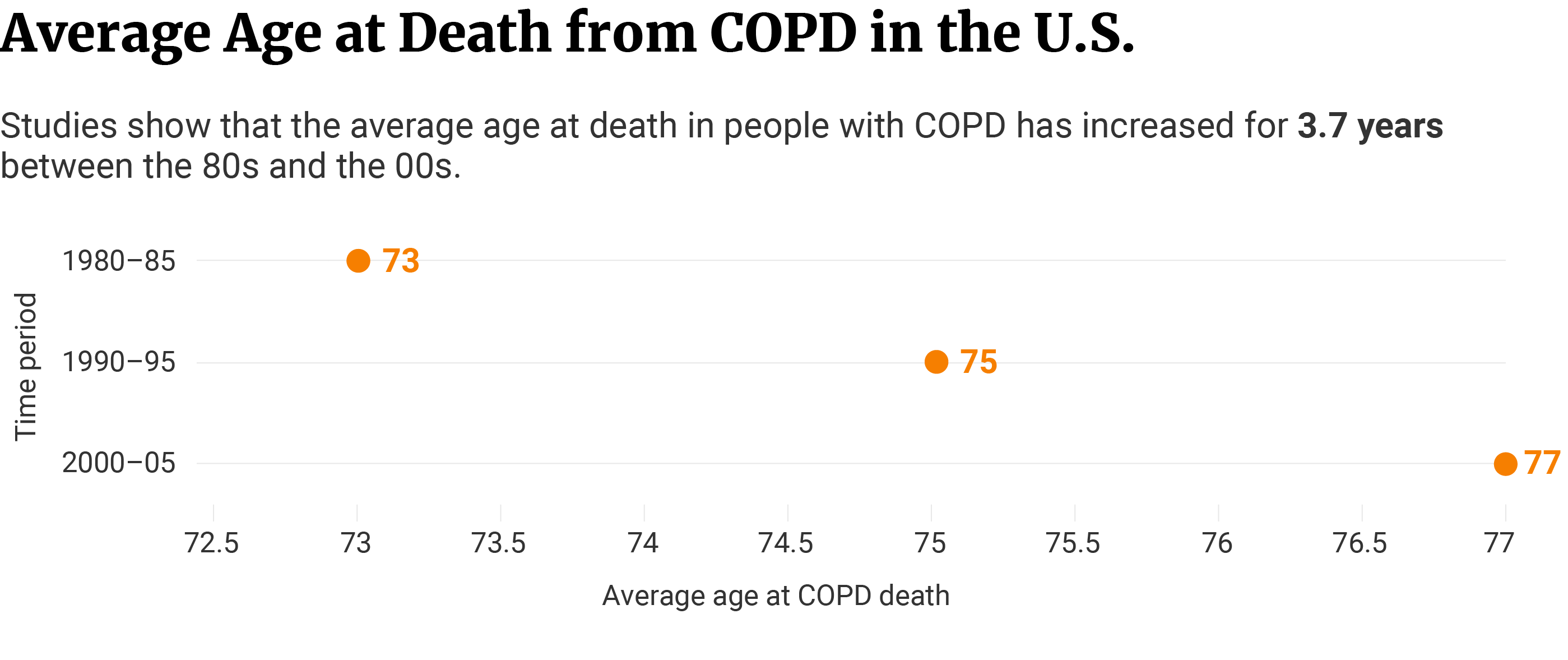

This data comes from the Journal of Chronic Obstructive Pulmonary Disease, which states that there was an increase in the average age at COPD death for three to four years between 1980 and 2005 [4].
What Is the Most Common Cause of Death in COPD Patients?
Studies show that 75% of COPD deaths are attributed to cigarette smoking [9]. This is unsurprising as one in five smokers will develop COPD throughout their lives [33].
Despite the danger COPD presents, data shows that 38% of the nearly 16 million U.S. adults with a COPD diagnosis are current smokers [31].
The fact that puzzles researchers is that 25% of the people who die of COPD have never smoked in their life [9].

People who have never smoked have a 67% lower COPD prevalence. The prevalence of COPD is also lower in former cigarette users at 43% and in cigar users at 54% [37].
Former cigarette users have a 72% higher prevalence of COPD compared to people who have never smoked cigarettes [37].
A study published in BM Pulmonary Medicine investigated the exclusive use of cigarettes within the past 30 days. It revealed that tobacco smoke is fundamental for the development and progression of COPD [37].
COPD Deaths Demographics
Of the 152,657 COPD deaths in 2020, women make up the most with 79,715 people. COPD deaths are also the highest among older people aged 75-79 with 25,311 and Whites with 130,947 [5].
COPD Deaths Statistics: Male vs. Female
More women died of COPD (79,715) than men (72,942) in 2020, says data from the Centers for Disease Control and Prevention [5].
The percentage of COPD deaths is higher in females at 52.22% than in males at 47.78%, but men have 9.3 lower percentage points of survival than women. Studies show that male COPD patients who are intubated are more likely to die in the long run than female patients [45].
The crude death rate per 100,000 people is 47.7 for females compared to 45.0 for males [5].
The crude death rate indicates the number of COPD deaths during the year per 100,000 midyear population.

Females with severe COPD have a 50% increased risk of hospitalization and a greater risk of death from respiratory complications than males. Females’ lung anatomy, low estrogen levels, and late diagnosis may be important risk factors for these, says a study published in the American Journal of Respiratory and Critical Care Medicine [2].
But, males have a historically higher exposure to smoke from cigarettes and occupational lung irritants as potential COPD risk factors for worse long-term survival [45]. Occupational exposure to lung irritants for COPD causes higher proportional mortality in males than females at a population attributable fraction of 10.6% and 6.1%, respectively [16].
COPD Deaths by Age Statistics
In 2020, most (84.31%) COPD deaths occurred among adults aged 65 years or older at a total of 128,712 [5].
25,311 older adults aged 75 through 79 years died of COPD in 2020. This age group also holds the highest percentage of deaths among all age groups at 16.58%. Older adults aged 80 through 84 follow with 24,052 deaths or 15.76% [5].
14.61% of older adults aged 70 to 74 years died of COPD in 2020, which equals 22,307 deaths. Older adults 85 through 89 are also in the top five age groups for COPD deaths at 13.60% or 20,766 deaths, followed by 65 through 69 year olds at 16,252 deaths or 10.65% [5].
Both the number of COPD deaths and the percentage fall proportionally in younger adults [5].
8.02% or 12,237 of COPD deaths in 2020 happened in adults 60 through 64 years, which is a difference of 4,015 deaths from the 65 through 69 age group. From there, the number of deaths notices nearly a double decline at 6,579 deaths (4.31%) in adults aged 55 through 59 years [5].
The lowest number of deaths in adults over 45 was in COPD patients aged 45 through 49 at 1,038 (0.68%). The 50 through 54 age group follows with 2,500 deaths or 1.64% [5].
In 2020, older adults aged 80 through 84 years had the highest death rate at 372.1 per 100,000. For comparison, only 180 people aged 25 through 29 died of COPD in 2020 at a 0.8 rate per 100,000 [5].
This indicates that both the number and the rate of COPD deaths are closely related to age and are the highest in older adults.
COPD Deaths by Race Statistics
At 130,947 out of 152,657 COPD deaths in 2020, White Americans have the highest number of deaths, percentage of deaths (85.78%), and death rates (65.3 per 100,000). Black Americans come in second with 12,361 deaths or 8.10% of all COPD deaths in 2020 [5].
The number of deaths is lowest in American Indian and Alaska Natives (AIANs) at 861 or 0.56%. Asian Americans at 2,176 (1.43%), and Hispanics at 5,949 or 3.90% follow [5].
Out of all races, Hispanics have the lowest death rate at 9.7 per 100,000, while White Americans have the highest at 65.3. Despite the low number of deaths, AIANs also have a high death rate at 31.1 [5].
Whites are 4.1 times more likely to develop COPD than Hispanics. COPD’s prevalence in Hispanics is lower by both spirometry and clinical diagnosis at 41.6% compared to Whites at 54.2% [1].
The exact reason for this is largely unknown, but a London study suggests that it may be due to ethnic differences in cigarette consumption and potential ethnic susceptibility to this disease [15].
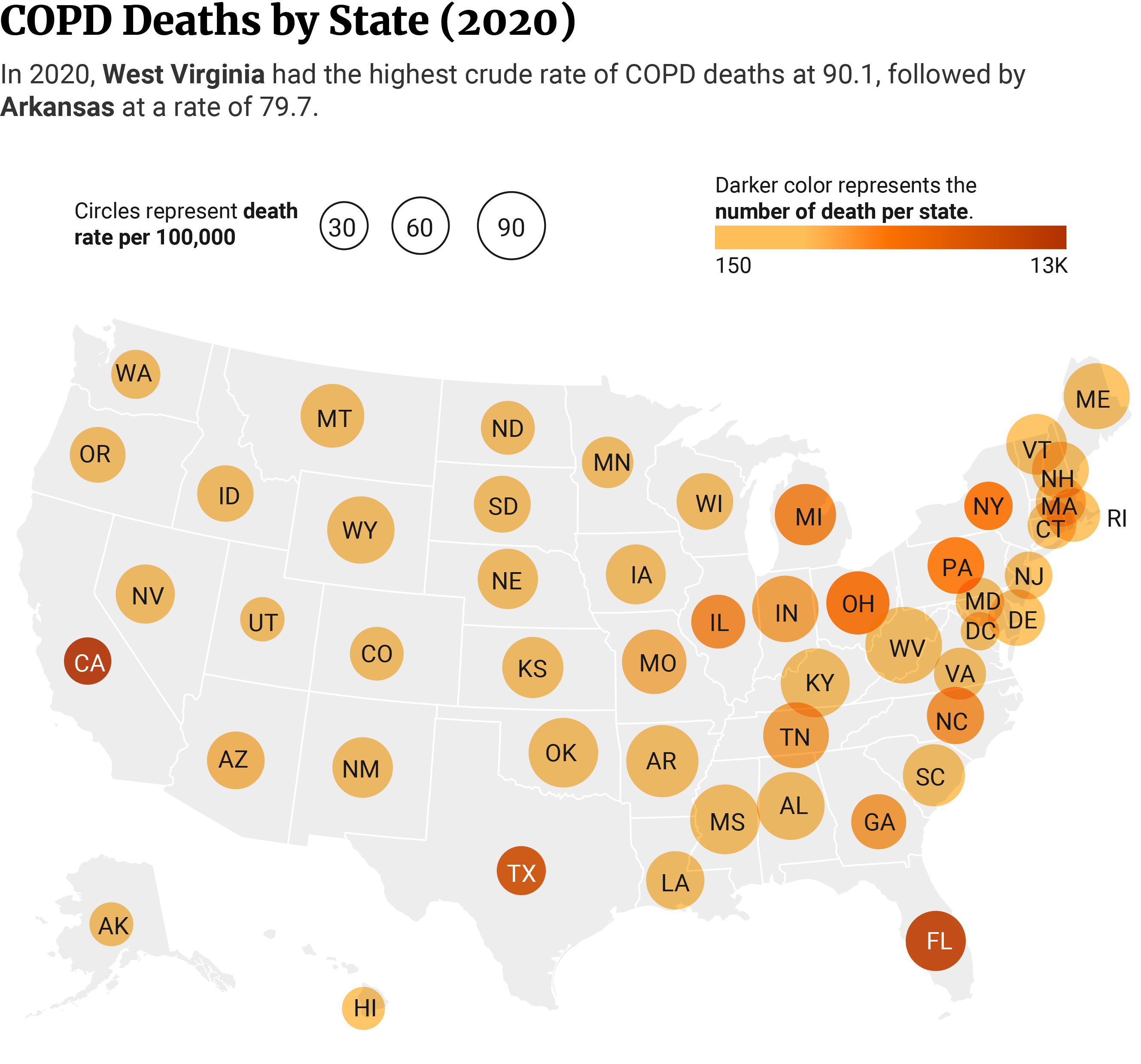
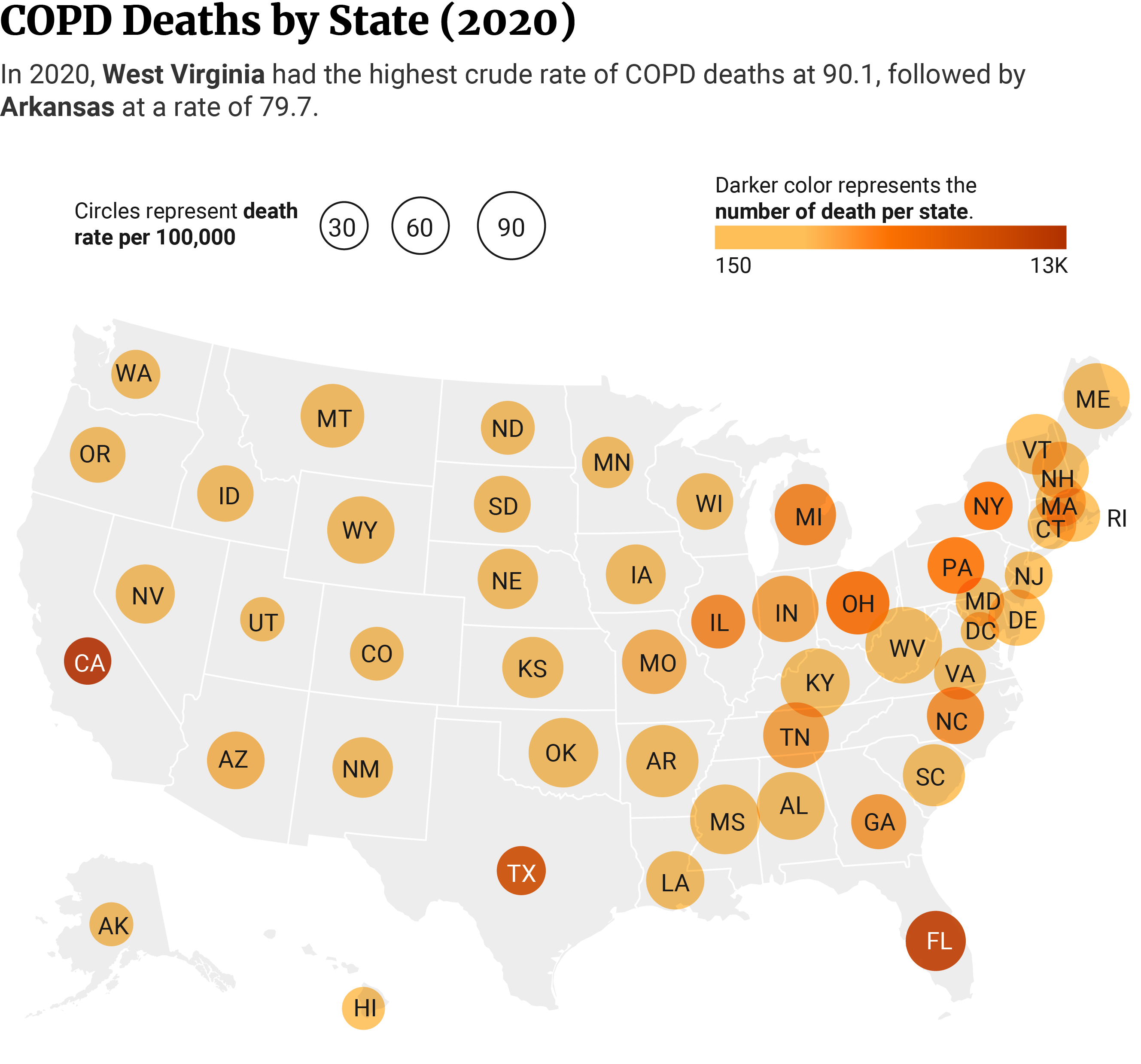
COPD Deaths by State Statistics
At 90.1 per 100,000, West Virginia had the highest COPD death rate, while Hawaii had the lowest at 26.7, shows 2020 data from the CDC [5].
West Virginia is the state with the highest percentage of tobacco use in the nation, with 23.8% of adult West Virginians being current smokers in 2022 [41].
Even though West Virginia had the highest COPD death rate and California is among the five states with lowest COPD death rate (32.8 per 100,000), California had the highest number of deaths at 12,907 or 8.45% out of all US states [5].
California is among the ten states with the lowest tobacco use rates, but it has the top four most polluted cities in the United States [27].
Second and third in line in the number of deaths were Florida (11,791) and Texas (10,402), respectively [5].
COPD Prevalence in the United States
COPD affects more than 15 million American adults, but the real number is greater because many people don’t know they have this condition [35].
In 2021, 4.6% of adults aged 18 and over suffered from emphysema or chronic bronchitis [32].
Data shows that more than half of the diagnosed adults are women [35].
COPD Prevalence Statistics: Male vs. Female
COPD is more prevalent in females at 7.1% than in males at 5.7%. Based on CDC sample data, women also have a higher number of COPD cases (19,989 out of 233,922) compared to men (14,180 out of 202,664) [3].
Biologically, women smokers are more susceptible to this disease because of the faster decline in FEV1 — even if smoking fewer cigarettes than men. Studies show that females develop more severe COPD and at an earlier age compared to males (younger than 60) [2].
Evidence shows that the 1960s propaganda by the tobacco industry that targeted women (and resulted in increased smoking rates) is partly to blame [18].
Another reason why women suffer from COPD more than men is that they are commonly misdiagnosed. COPD has been known for decades as a man’s disease, so female smokers are more than 33% less likely to be diagnosed with COPD compared to male smokers [18].
Cumulatively, women consume less tobacco than men but are more susceptible to it, resulting in a more severe, earlier-onset COPD and a faster FEV1 decline. The numbers show that women represent 80% of the nonsmoker COPD patient group, likely due to biomass fuel exposure or indoor air pollution created by poorly ventilated areas for cooking [18].
Note: The FEV1 measures how quickly the lungs are emptied after taking a maximal inhale. An excessive decline of this parameter over the course of 5 or more years is tightly correlated to the level of lung function and a predictor of morbidity and mortality. At a normal rate, the FEV1 decline should be 30 ml/y [44].
COPD Prevalence by Age Statistics
With 5,381 cases, the 70 to 74 age group has the highest number of people with COPD. It’s followed by the 65 to 69 group at 4,998 cases and the 60 to 64 age group at 4,826 cases [3].
The highest prevalence rate of COPD cases by age is in adults aged 75 to 79 at 13.8%. Adults aged 70 to 74 follow at 13.2%, and older than 80 at 12.6% [3]. The prevalence rate of COPD significantly increases with age.
Only 1.7%, or 410 people aged 18 to 24, have ever been told they had COPD, which remains the age group with the lowest prevalence and lowest number of cases. The 25 to 29 age group and the 30 to 34 age group follow with 464 (2.3%) and 632 (3.0%) cases, respectively [3].
Smokers are most likely to suffer from COPD, but this condition is most common in people older than 40 who are smokers or have smoked earlier in life [34].
While young adults can, but rarely, develop COPD, the first symptoms appear in adults who are at least in their forties [10].
COPD Prevalence by Race Statistics
COPD affects American Indian and Alaskan Natives (AIAN) the most at 10.6% or 720 cases out of 7,214 people. At 7.9% or 901 and 7.6% or 27,865 cases, Multiracial Americans and White Americans, respectively, follow [3].
Black Americans are the fourth most commonly affected race from COPD based on CDC’s sample size at 6.3% [3].
White Americans have the highest number of COPD cases at 27,865 out of 330,730 people. Black Americans come in second at 2,386 COPD cases out of 32,946 people. Hispanics are third with 1,566 cases out of 38,230 people [3].
This may be connected to high smoking rates among AIANs at 27.1% compared to Asians and Hispanics at 8.0% each, and the overall US population at 12.5% or 30.8 million people [30].
In 2020, American Indians and Alaska Natives (AIANs) had the highest smoking prevalence compared to other races in the US [30].
This group tends to hold sacred tobacco ceremonials, and use tobacco for religious and medical uses. Also, tobacco sold in their lands is not taxed, so that’s another contributor to increased tobacco smoking rates [30].
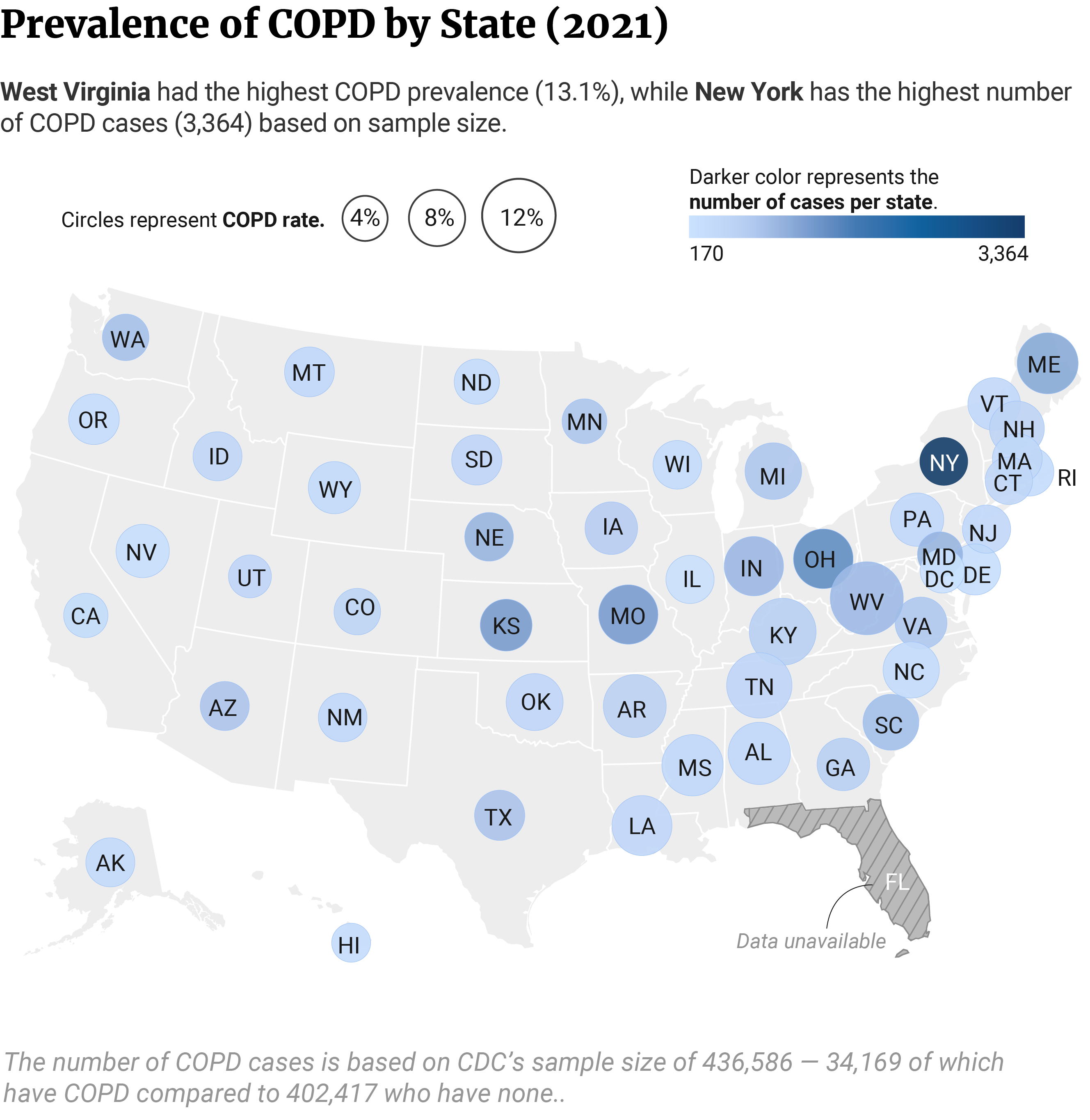
COPD Prevalence by State Statistics
Based on CDC’s sample size, New York has the highest number of COPD cases at 3,364. Ohio and Kansas follow at 1,500 and 1,310 cases, respectively [3].
The states with the lowest number of COPD cases are Illinois with 211, Nevada with 255, and Delaware with 277 [3].
West Virginia has the highest prevalence rate by state. Out of 6,711 West Virginians, 13.1% or 951 have been told they had COPD at any time of their lives, followed by 10.9% or 699 out of 5,395 Kentuckians [3].
Tennessee and Arkansas are also among the top five states with the highest COPD prevalence by state. 10.4% or 529 people out of 4,763 Tennesseans and 9.6% or 646 people out of 5,349 Arkansans have been told they had COPD at any time in their lives [3].
The state with the lowest COPD prevalence by cases is Hawaii, with 3.5% or 346 cases out of 7,768 people, followed by Utah at 4.3% or 543 cases out of 10,546 [3].

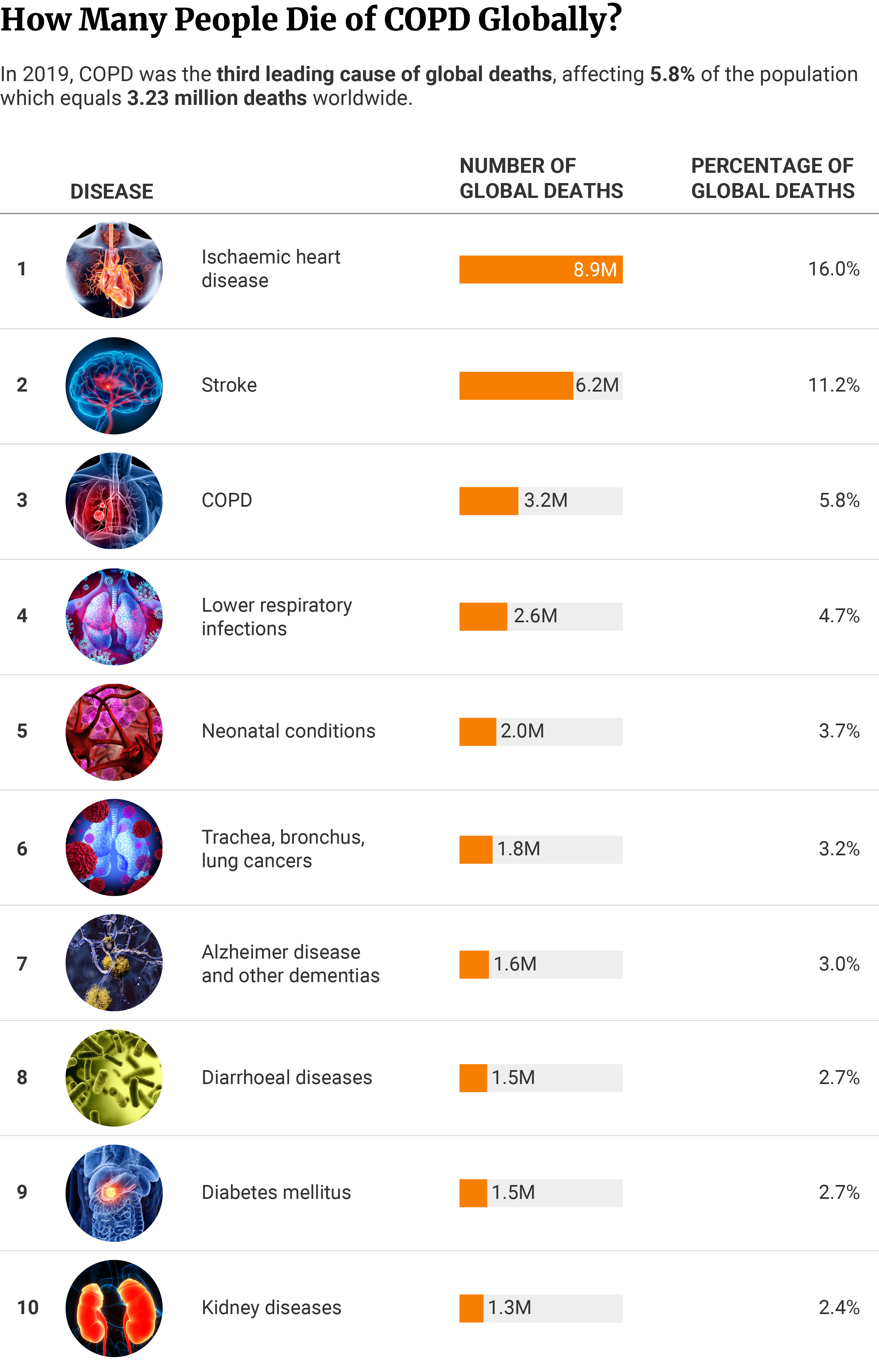
COPD Statistics — Deaths Worldwide
In 2019, 3.23 million people, or 5.8% of global deaths were attributed to COPD. This disease was the third leading cause of death worldwide after ischaemic heart disease with 8.89 million deaths (16.0%) and stroke with 6.19 million (11.2%) [12] [13].
Global and regional estimates show that lower respiratory infections, neonatal conditions, and Alzheimer's were among the ten leading causes of death globally in that year [13].
Diabetes mellitus (1.5 million) and kidney disease (1.33 million) were at the bottom of the list of leading causes of global deaths [12].

Most Common Causes of COPD in Non-Smokers
53.9% out of 200 non-smoking COPD patients developed this condition due to exposure to biomass smoke, says an Indian study. Treated pulmonary tuberculosis was a significant risk factor in 32.7% of the non-smoking patients and long-standing asthma in 14.2% of the patients [38].
Ten percent (10%) of the non-smoking patients developed COPD due to several risk factors, including occupational exposure, outdoor air pollution exposure, and lower respiratory tract infection in childhood [38].
Up to 30% of people with COPD are non-smokers and have never smoked in their lives [35]. Here are a few more answers to why non-smokers develop COPD.
![]()

Poor Lung Development
Out of 200 non-smoking COPD patients, 28.9% suffered more respiratory infections during childhood compared to 18.7% of smokers, shows data from a Korean multicenter cohort [6].
According to researchers, the reason why people who never smoked develop COPD may be improper lung development [24]. Research has shown that even at an early age, older adults with COPD appear to have experienced low lung function. Although unconfirmed, frequent respiratory infections during childhood may explain why non-smokers have experienced low function at an early age [6].
At 57.5% out of 2,477 patients, females comprise a higher proportion of non-smoking COPD patients compared to smoking COPD patients at 3.3% [6]. A strong risk factor for COPD in non-smokers is small airways relative to lung size, says a 2020 JAMA study [24].
Females have relatively smaller airways than males, but the reasons why females with small airways have a greater susceptibility to COPD is unknown. One theory is that the concentration of tobacco smoke may be greater per unit area in a smaller airway surface, but this remains to be investigated [2].
Secondhand Smoke (SHS)
Among 334 COPD patients who don’t actively smoke, 66.65% were exposed to short-term and 34.91% to medium-term secondhand smoke, showed a five-year survey by the US National Health and Nutrition [14].
The short term SHS exposure in COPD patients who don’t actively smoke was 3.73 times higher compared to the general population of adult nonsmokers older than 40 [14].
![]()

A significant contributor to COPD in people who don’t smoke and have never smoked is long-term exposure to secondhand smoke [31].
In addition, people who have been exposed to secondhand smoke during childhood and teenage years are at a greater risk of developing COPD in their adult years. This is because exposure to secondhand smoke in children and teens can slow the process of lung growth and development [31].
AATD Deficiency
One to four percent of COPD patients have a rare, hereditary genetic condition known as alpha-1-antitrypsin deficiency (A1AD) [26]. According to the British Lung Foundation, having AATD increases the likelihood of the patient developing COPD [48].
Research shows that AATD remains underdiagnosed in COPD patients, despite recommendations to check for it in these patients [25].
COPD patients 40 years of age or older have an adjusted rate of AATD of 0.83% [25].
What Are the Stages of COPD?
The stages of COPD are based on the Global Initiative for Chronic Obstructive Lung Disease (GOLD) Guidelines. The GOLD guidelines put COPD development in four stages, including mild, moderate, severe, and very severe [43].
At Stage I of the disease (mild), the person may experience no symptoms but typically has difficulty breathing when walking the stairs. Their airflow is 80% of the normal airflow [42].
At Stage II, or the moderate stage, the person experiences symptoms like chronic cough, breathlessness, or wheezing and needs breaks to catch their breath. Their airflow is within the 50% to 79% range compared to normal levels [42].
At Stage III or the severe stage, the person experiences worsening symptoms. The shortness of breath is greater, and further exacerbations affect the person’s quality of life and may lead to hospitalization. Their airflow remains within the 30% to 50% range of normal levels [42].
At Stage IV, or the very severe stage, the situation becomes alarming because the person’s airflow is less than 30% compared to normal levels. The person experiences severe airflow limitation, and further exacerbations can be life-threatening [42].
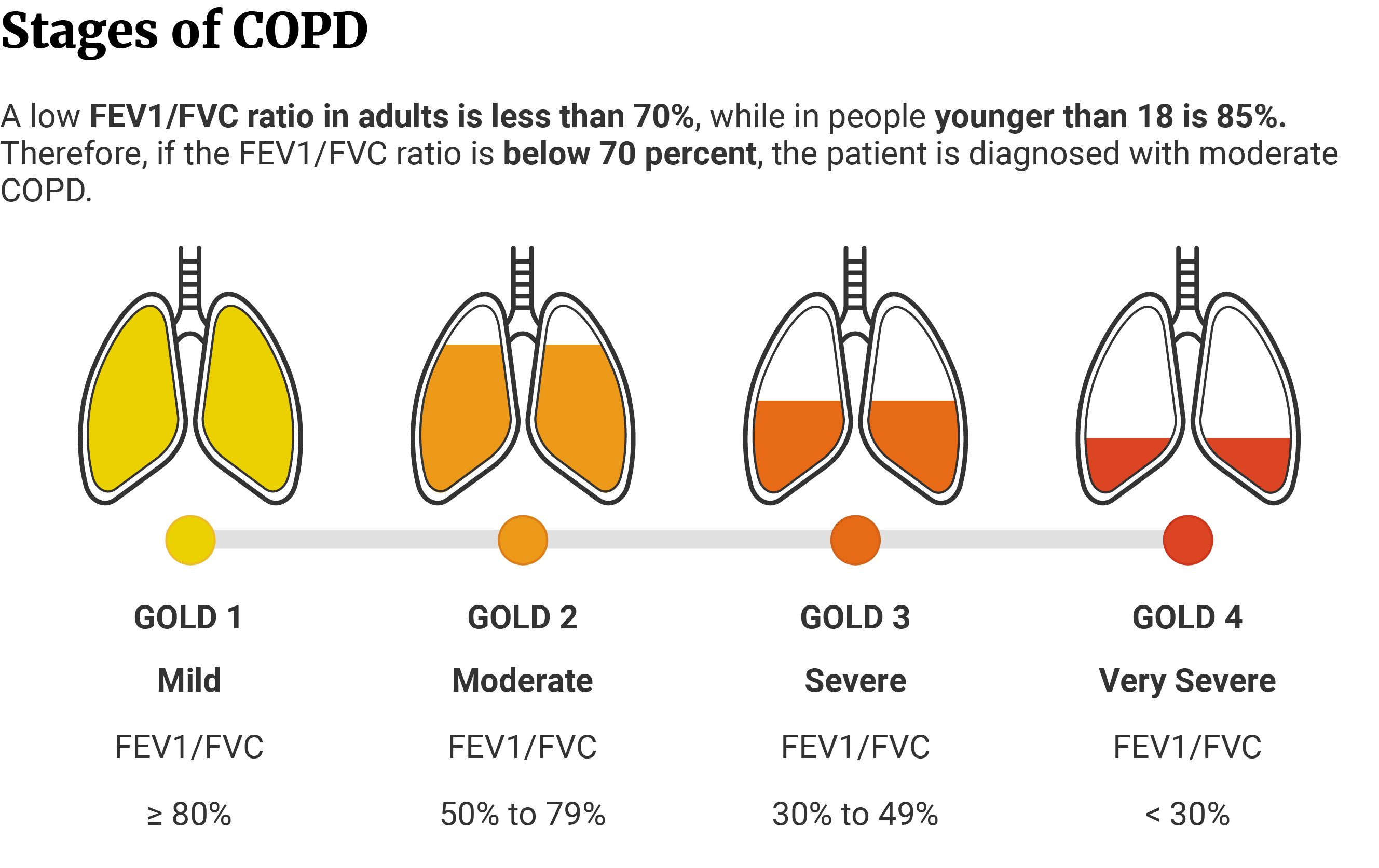

Physicians use these four stages to determine the severity of COPD in the patient and help pair them with the right treatment for their stage [43].
The entire classification is based on two parameters: Forced vital capacity (FVC) and Forced expiratory volume (FEV1) [43].
The FVC parameter measures the largest amount of air the patient can breathe out after taking the deepest breath. The FEV1 parameter measures how much air the patient can exhale from the lungs in 1 second [43].
Every patient has an individual predicted FEV1 value. Once calculated, the doctor compares the predicted value to the actual FEV1 score and its ratio to FVC [43].
How Many Years of Smoking Does It Take to Develop COPD?
After 25 years, 30-40% of smokers will develop any COPD, while at least 25% of completely healthy smokers will develop COPD described as clinically significant [23].
![]()

![]()
The data came from a Dutch study that followed men and women who smoked (but had normal lung function) for 25 years that concluded that the longer people smoked, the greater the risk of developing COPD [23].
What’s The Average Life Expectancy for People Diagnosed with COPD?
The average life expectancy in relatively healthy 65-year-old Caucasian males with COPD is 17.4 years at Stage 1 of the disease and 12.5 years at Stage 3 or 4 [39].
Relatively healthy 65-year-old Caucasian females with COPD have an average life expectancy of 19.9 years at Stage 1 of the disease and 14.5 years at Stage 3 or 4 [39].
In conclusion, females diagnosed with COPD have a higher average life expectancy than males [39].
Data shows that people diagnosed with COPD who continue to smoke have the lowest average life expectancy [39].
Current male smokers have the lowest average life expectancy of 8.5 years at Stage 3 or 4 of the disease, while current female smokers have an average life expectancy of 11.3 years at the same stage [39].
Life Expectancy Highest in Never Smokers
In never smokers, there’s a tiny drop in average life expectancy by 0.7 and 1.3 years at stages 2 and 3 of COPD, respectively [39].
Compared to smokers, people who have never smoked but were diagnosed with COPD noticed a moderate decline in life expectancy. Current and former smokers experience a significant reduction in life expectancy from COPD [39].
COPD Average Life Expectancy Chart
The average life expectancy in people who never smoke is higher than in people diagnosed with COPD who are current and former smokers [39].
- Compared to never smokers, 65-year old current male and female smokers diagnosed with COPD have a reduced life expectancy of 0.3 and 0.2 years at stage 1, respectively. At stage 2, life expectancy is reduced by 2.2 years in both male and female current smokers. At stage 3 or 4, the life expectancy is greatly reduced compared to never smokers at 5.8 years in current male smokers and 6.1 years in current female smokers.
- Former male smokers have a reduced life expectancy of 1.4 years and 5.6 years for Stages 2, and 3 or 4, respectively.
- Former female smokers have a reduced life expectancy of 2 and 6.3 years for stages 2, and 3 or 4, respectively.
In addition to the reduction in life expectancy of COPD, current smokers also lose an additional 3.5 years of their lives due to smoking [39].
What’s The Survival Rate of COPD?
Hospitalized COPD patients are 82% less likely to survive within the next 15 years compared to the general population [46].
Patients who experience worsening COPD are 7.3% likely to survive the next 15 years compared to the general population at 40.6% [46].
The survival rate in COPD patients depends on the GOLD stage of the disease [46].
COPD patients in the GOLD I stage have a 15-year survival of 24.0% compared to 11.1% and 5.3% survival at GOLD stages II and III, respectively [46].
43.7% of patients will survive the 5-year mark after COPD exacerbation, and 19.9% will survive a decade compared to 57.2% of the general population [46].
COPD patients have a reduced overall 15-year survival after diagnosis at an early stage and an even lower survival after hospitalization and exacerbation of symptoms [46].
This data is based on a study published in Respiratory Medicine that studied the mortality risks of people diagnosed with COPD — including hospitalized COPD patients versus subjects from the general population [46].
When undergoing non-invasive ventilation (NIV) treatment, women showed a survival tendency at a survival rate of 25.7%, compared to men at 19.2% [45].
A study published in the International Journal of Chronic Obstructive Pulmonary Disease treated patients with non-invasive ventilation (NIV) for acute respiratory failure for the first time. The study was conducted at a university hospital in Denmark on 253 patients at a median age of 72 years [45].
In general, patients with acute respiratory failure don’t leave long after receiving NIV. This study noted a 30-day mortality rate of 29.3% and a survival rate of 23.7% [45].
What's the Annual Cost of COPD?
The US spent an estimated $49 billion in 2020, an increase from 2010s $32.1 billion. It's a costly condition, especially due to the high rate of hospitalization among older adults over 65 [29].
51% of the annual 2010 COPD costs went to Medicare, and 18% were covered by private insurance [29]. The annual cost of COPD was three times higher in patients with severe COPD ($18,070) compared to patients with mild COPD ($5,945) [19].
In 2010, this condition caused a loss of 16.4 million days of work at the cost of $3.9 billion [29].
COPD is expensive, but luckily, the Social Security Administration (SSA) considers it a disability. If you’re not able to work due to advanced COPD, the SSA has a few assistance programs to help with the payments. Severe enough stages of COPD that don’t allow you to work for at least 12 months mean you’ll likely qualify for disability [7].
How Long Does It Take to Get Disability for COPD?
On average, it takes three to five months to find out whether the person qualifies for a disability for COPD. After getting approved, it takes another five months until the person receives their first disability benefit payment [7].
![]()

![]()

Common Treatments for COPD
While there’s no proven cure for COPD, several treatment options have shown more or less effective in treating this condition.
Amoxicillin/Clavulanic Acid
74.1% or 117 patients with nonsevere worsening of mild to moderate COPD improved on a combination of amoxicillin and clavulanic acid compared to placebo at 59.9% or 91 patients [22].
The patients who participated in this multicenter trial took a dosage of 500/125 mg amoxicillin/clavulanic acid three times a day for eight days and noticed a prolonged time between the last and the next interval of acute exacerbation of mild to moderate COPD (AECOPD) [22].
Corticosteroids
Four-week treatment with a high dose of oral steroids (over 30 mg) improves lung function in some COPD patients by up to 20% [17].
The researchers noted a significant improvement in patients’ FEV1 after two weeks of this treatment. However, they concluded that such high doses of corticosteroids are unsustainable in the long run due to the harm they do to the body [47].
Salmeterol/Fluticasone Combination
A salmeterol/fluticasone blend reduced the exacerbations in moderate and severe COPD cases but there was still a 64% increase in the risk of developing pneumonia compared to placebo [11].
The researchers have concluded that an extra case of pneumonia will develop for every 31 patients undergoing this therapy over a year [11].
In an attempt to improve COPD treatment and reduce the appearance of pneumonia as an adverse event, researchers studied the impact of a corticosteroid combination. The patients took part in a three year study and were treated with fluticasone alone or a combination of salmeterol and fluticasone [11].
Multifactorial Intervention
56.8% out of 146 patients diagnosed with COPD had reduced mobility impairment and 23.7% experienced increased cognition after a multifactorial intervention. The trial consisted of 91.8% male patients at a mean age of 69.8 years [21].
A study published in BM Pulmonary Medicine evaluated the effectiveness of a multifactorial intervention in COPD patients with scheduled inhalation therapy. This intervention included multiple components such as [21]:
- Information on COPD
- Training in inhalation techniques
- Audio-visual materials
- Dose reminders
- Motivational aspects
Carbocysteine
Carbocysteine therapy decreases acute exacerbations in patients with COPD by 24% compared to placebo. The participants of the study took 1500 mg of this mucolytic for a year [36].
Final Thoughts — COPD Facts & Statistics
Chronic obstructive pulmonary disease (COPD) affects nearly 16 million Americans and is the cause of over 150,000 deaths per year. Smoking is the root cause of COPD, with cigarette smoking causing about 75% or nearly 8 out of 10 deaths.
Adults 75 and older have the highest number and rate of COPD deaths. Only 7.3% of the patients diagnosed with COPD will survive the next 15 years after admission for worsening COPD.
Once hospitalized, COPD patients at Stage I have a 24% chance of survival within the next 15 years compared to patients at Stage III at 5.3%. Treating chronic pulmonary obstructive disease is costly and amounts to 16.4 million days of total absenteeism.
References
- Aiyer, A., Surani, S., Aguillar, R., Sharma, M., Ali, M., & Varon, J. (2020). Ethnic Variance in Prevalence of COPD among Smokers in a Real World Setting. The Open Respiratory Medicine Journal, 14, 93–98. [1]
- Barnes, P. J. (2016). Sex Differences in Chronic Obstructive Pulmonary Disease Mechanisms. American Journal of Respiratory and Critical Care Medicine, 193(8), 813–814. [2]
- Behavioral Risk Factor Surveillance System. (2022). Centers for Disease Control and Prevention. [3]
- Brown, D. W., Croft, J. B., Greenlund, K. J., & Giles, W. H. (2009). Average Age at Death from COPD in the United States: 1980–85, 1990–95, 2000–05. COPD: Journal of Chronic Obstructive Pulmonary Disease, 6(3), 152–154. [4]
- CDC Wonder. (2022). Centers for Disease Control and Prevention. [5]
- Choi, J. Y., Kim, J. W., Kim, Y. H., Yoo, K. H., Jung, K. S., Lee, J. H., Um, S. J., Lee, W. Y., Park, D., & Yoon, H. K. (2022). Clinical Characteristics of Non-Smoking Chronic Obstructive Pulmonary Disease Patients: Findings from the KOCOSS Cohort. COPD: Journal of Chronic Obstructive Pulmonary Disease, 19(1), 174–181. [6]
- Chronic Obstructive Pulmonary Disease and Social Security Disability. (2021). Disability Benefits Help. [7]
- Chronic obstructive pulmonary disease (COPD). (2022). World Health Organization. [8]
- COPD. (2022). Centers for Disease Control and Prevention. [9]
- COPD Causes and Risk Factors. (2018). COPD Foundation. [10]
- Crim, C., Calverley, P. M. A., Anderson, J. A., Celli, B., Ferguson, G. T., Jenkins, C., Jones, P. W., Willits, L. R., Yates, J. C., & Vestbo, J. (2009). Pneumonia risk in COPD patients receiving inhaled corticosteroids alone or in combination: TORCH study results. European Respiratory Journal, 34(3), 641–647. [11]
- Elflein, J. (2022a). Leading causes of death worldwide 2019. Statista. [12]
- Elflein, J. (2022b). Leading ten causes of death in the world 2019. Statista. [13]
- Fu, Z., Jiang, H., Xu, Z., Li, H., Wu, N., & Yin, P. (2020). Objective secondhand smoke exposure in chronic obstructive pulmonary disease patients without active smoking: the U.S. National Health and Nutrition Examination Survey (NHANES) 2007–2012. Annals of Translational Medicine, 8(7), 445. [14]
- Gilkes, A., Ashworth, M., Schofield, P., Harries, T. H., Durbaba, S., Weston, C., & White, P. (2016). Does COPD risk vary by ethnicity? A retrospective cross-sectional study. International Journal of Chronic Obstructive Pulmonary Disease, 11, 739–746. [15]
- Grahn, K., Gustavsson, P., Andersson, T., Lindén, A., Hemmingsson, T., Selander, J., & Wiebert, P. (2021). Occupational exposure to particles and increased risk of developing chronic obstructive pulmonary disease (COPD): A population-based cohort study in Stockholm, Sweden. Environmental Research, 200. [16]
- Grimes, G. C., Manning, J. L., Patel, P., & Via, R. M. (2007). Medications for COPD: A Review of Effectiveness. American Family Physician, 76(8), 1141–1148. [17]
- Gut-Gobert, C., Cavaillès, A., Dixmier, A., Guillot, S., Jouneau, S., Leroyer, C., Marchand-Adam, S., Marquette, D., Meurice, J. C., Desvigne, N., Morel, H., Person-Tacnet, C., & Raherison, C. (2019). Women and COPD: do we need more evidence? European Respiratory Review, 28(151), 180055. [18]
- Larsen, D. L., Gandhi, H., Pollack, M., Feigler, N., Patel, S., & Wise, R. (2022). The Quality of Care and Economic Burden of COPD in the United States: Considerations for Managing Patients and Improving Outcomes. American Health and Drug Benefits, 15(2), 57–64. [19]
- Lee, Y. C., Chang, K. Y., & Sethi, S. (2021). Association of Chronic Lower Respiratory Disease With County Health Disparities in New York State. JAMA Network Open, 4(11), e2134268. [20]
- Leiva-Fernández, J., Leiva-Fernández, F., García-Ruiz, A., Prados-Torres, D., & Barnestein-Fonseca, P. (2014). Efficacy of a multifactorial intervention on therapeutic adherence in patients with chronic obstructive pulmonary disease (COPD): a randomized controlled trial. BMC Pulmonary Medicine, 14, 70. [21]
- Llor, C., Moragas, A., Hernández, S., Bayona, C., & Miravitlles, M. (2012). Efficacy of Antibiotic Therapy for Acute Exacerbations of Mild to Moderate Chronic Obstructive Pulmonary Disease. American Journal of Respiratory and Critical Care Medicine, 186(8), 716–723. [22]
- Løkke, A., Lange, P., Scharling, H., Fabricius, P., & Vestbo, J. (2006). Developing COPD: a 25 year follow up study of the general population. Thorax, 61(11), 935–939. [23]
- Lung development may explain why some non-smokers get COPD and some heavy smokers do not. (2020). National Institutes of Health. [24]
- Menga, G., Fernandez Acquier, M., Echazarreta, A. L., Sorroche, P. B., Lorenzon, M. V., Fernández, M. E., & Saez, M. S. (2020). Prevalence of Alpha-1 Antitrypsin Deficiency in COPD Patients in Argentina. The DAAT.AR Study. Archivos De Bronconeumología, 56(9), 571–577. [25]
- Monge, M. B., Silva, R., Czischke, K., Saldías, F., Pavié, J., Jalón, M., Benavides, M. G., San Martín, B., Cea, X., Mendoza, L., Roldán, R., Soto, L., De La Prida, M., Zambrano, A., Villalobos, J., Gutiérrez, M., Riquelme, M., Tapia, M., & Dreyse, J. (2021). Prevalence of alpha-1-antitrypsin deficiency (A1AD) in patients with COPD. European Respiratory Journal, 58(65). [26]
- Most Polluted Places to Live. (2022). American Lung Association. [27]
- National Center for Chronic Disease Prevention and Health Promotion. (2015). Chronic Obstructive Pulmonary Disease (COPD). Centers for Disease Control and Prevention. [28]
- National Center for Chronic Disease Prevention and Health Promotion. (2018). COPD Costs. Centers for Disease Control and Prevention. [29]
- National Center for Chronic Disease Prevention and Health Promotion. (2022a). Burden of Cigarette Use in the U.S. Centers for Disease Control and Prevention. [30]
- National Center for Chronic Disease Prevention and Health Promotion. (2022b). Smoking and COPD. Centers for Disease Control and Prevention. [31]
- National Center for Health Statistics. (2022). Percentage of COPD, emphysema, or chronic bronchitis for adults aged 18 and over, United States, 2021. National Health Interview Survey. [32]
- National Heart, Lung, and Blood Institute. (2017). COPD National Action Plan. National Institutes of Health. [33]
- National Heart, Lung, and Blood Institute. (2018). COPD: The More You Know, The Better For You and Your Loved Ones. In National Institutes of Health (No. 13–5840). [34]
- National Heart, Lung, and Blood Institute. (2021). What Is COPD? National Institutes of Health. [35]
- Pace, E., Cerveri, I., Lacedonia, D., Paone, G., Sanduzzi Zamparelli, A., Sorbo, R., Allegretti, M., Lanata, L., & Scaglione, F. (2022). Clinical Efficacy of Carbocysteine in COPD: Beyond the Mucolytic Action. Pharmaceutics, 14(6), 1261. [36]
- Paulin, L. M., Halenar, M. J., Edwards, K. C., Lauten, K., Stanton, C. A., Taylor, K., Hatsukami, D., Hyland, A., MacKenzie, T., Mahoney, M. C., Niaura, R., Trinidad, D., Blanco, C., Compton, W. M., Gardner, L. D., Kimmel, H. L., Lauterstein, D., Marshall, D., & Sargent, J. D. (2022). Association of tobacco product use with chronic obstructive pulmonary disease (COPD) prevalence and incidence in Waves 1 through 5 (2013–2019) of the Population Assessment of Tobacco and Health (PATH) Study. Respiratory Research, 23, 273. [37]
- Sharma, B. B., & Singh, V. (2017). Nonsmoker COPD: Is it a reality? Lung India, 34(2), 117–119. [38]
- Shavelle, R. M., Paculdo, D. R., Kush, S. J., Mannino, D. M., & Strauss, D. J. (2009). Life expectancy and years of life lost in chronic obstructive pulmonary disease: Findings from the NHANES III Follow-up Study. International Journal of Chronic Obstructive Pulmonary Disease, 4, 137–148. [39]
- Smoking and Respiratory Diseases. (2022). Centers for Disease Control and Prevention. [40]
- Smoking Rates by State 2022. (2022). World Population Review. [41]
- Stages of COPD and Spirometric Classifications. (2008). Oklahoma Department of Human Services. [42]
- Summarizing the 2021 Updated GOLD Guidelines for COPD. (2021). US Pharmacist. [43]
- The National Institute for Occupational Safety and Health. (2011). Spirometry Quick calculation of FEV1 decline. Centers for Disease Control and Prevention. [44]
- Titlestad, I. L., Lassen, A. T., & Vestbo, J. (2013). Long-term survival for COPD patients receiving noninvasive ventilation for acute respiratory failure. International Journal of Chronic Obstructive Pulmonary Disease, 8, 215–219. [45]
- van Hirtum, P. V., Sprooten, R. T. M., van Noord, J. A., van Vliet, M., & de Kruif, M. D. (2018). Long term survival after admission for COPD exacerbation: A comparison with the general population. Respiratory Medicine, 137, 77–82. [46]
- Walters, J. A., Walters, E. H., & Wood-Baker, R. (2005). Oral corticosteroids for stable chronic obstructive pulmonary disease. Cochrane Database of Systematic Reviews, 3. [47]
- What is A1ATD? (2013). Asthma and Lung UK. [48]
